If you’ve been meaning to ask “Tell me something interesting about the B-17 Flying Fortress,” then today is your day.
 |
The B-17 was a heavy bomber, first built in 1935, that played a major role in World War II, especially in the campaign of daylight bombing against Nazi Germany.
It was horrific duty, in which anoxia, frostbite, and burns supplemented gunfire as physical threats to the 10-man crews. Half of all men suffered some degree of anoxia during their combat tours. More were disabled by frostbite than by gunfire – not surprising given the air temperatures of 30-to-50 below zero Fahrenheit, and the large openings in the side of the fuselage through which the waist gunners fired their weapons.
A normal tour was “only” 25 missions, but just 35% of aviators survived their tour (i.e. alive and not in German hands). On one raid against the heavily defended German city of Schweinfurt, 60 of 291 B-17s did not return – a 19% loss rate on one mission. Here is the mortality curve for all heavy bombers in Europe during World War II:
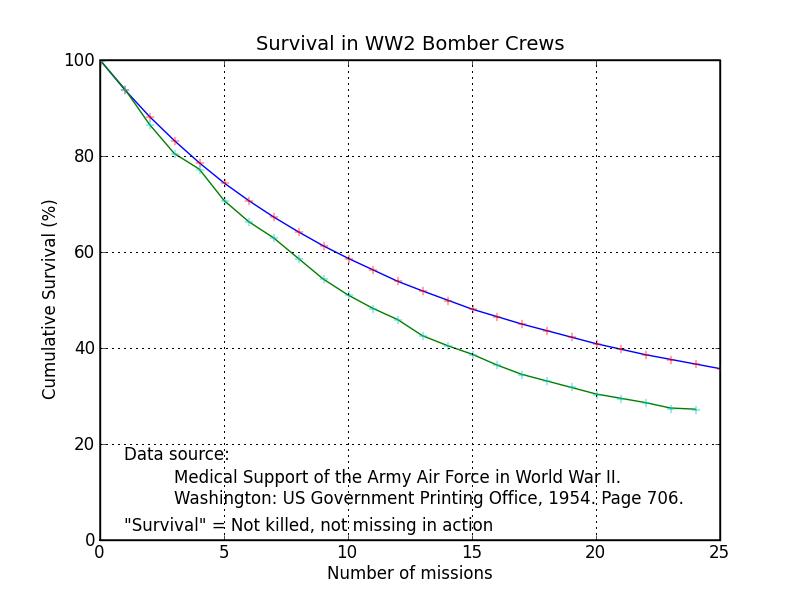 |
All told, the Air Force (then called the Army Air Force) suffered horrific casualties in its 3.75 years of European combat operations: 20,000 killed, 8400 wounded, and 35,000 missing (ref.: table 86). This does not include psychiatric casualties.
Fear was pervasive and severe. The traditional greeting for new arrivals at a bomber base was “You’ll be sorry,” without humor. Psychiatrists found that the effective men were able to convert fear into aggression. All feelings unrelated to combat drained away, and “No values existed other than those meaningful in combat.” Ninety-five per cent of crewmembers developed definite symptoms of “operational fatigue,” 34% suffering severely. At a special rest-and-relaxation base, aviators were routinely put into 3-day medical comas to break their stress.
Tragically, the losses were amplified by stupidity at the highest levels of the Air Force. Until late in the war, American fighters were not equipped with extra fuel tanks so they could protect the bombers all the way into Germany and back. Once they were – a simple fix – bomber missions became far more successful and far safer. Hermann Goering feared the war’s outcome was decided as soon as he saw the first American fighter over Germany.
Two utterly remarkable books can be highly recommended to anyone with even a small interest in the topic:
-
Decision Over Schweinfurt, by Thomas M. Coffey
-
Psychiatric Experiences of the Eighth Air Force: First Year of Combat (July 4, 1942 - July 4, 1943), by Donald W. Hastings; David G. Wright; Bernard C. Glueck
On a far lighter note, I’ve not seen it mentioned elsewhere that the B-17 ball turret must certainly have inspired the spaceship Discovery’s pods in the 1968 Stanley Kubrick film 2001: A Space Odyssey:
 |
The B-24 also used the same model of ball turret, according to this interesting web page. Here is another good picture of a ball turret module.
{kind=link}